#78 V-Tach Master Class with Dr. Sara Crager
Join us for this fun and exciting CCT episode where we are joined by the incredible Dr. Sara Crager for an all-expenses paid journey through the world of Ventricular Tachycardia! On this episode we explore the causes and pathophysiology of VT. Building upon that solid foundation, we also discuss different therapeutic approaches using a case-based format that's sure to leave a lasting impression. We hope you listen, learn and leave us a review! And if you feel so inclined, reach out on our socials and let us know what you think!

Sara Crager, MD
Dr. Sara Crager is an emergency physician, intensivist, educator, and founder of ICU.edu
Approach to Ventricular Tachycardia Storm
Big Picture: Two Major VT Phenotypes
The heart is the problem
The heart is innocent bystander
This distinction matters because the treatments are fundamentally different.
1. Structural Heart Disease ("The Heart Is the Problem")
Examples:
Prior myocardial infarction
Ischemic cardiomyopathy
Nonischemic cardiomyopathy
Ventricular scar
In these patients, the myocardium itself provides the substrate for VT.
Characteristics:
Usually monomorphic VT
Often caused by reentry circuits
Frequently recurrent
Often requires definitive EP intervention
2. The Heart as an "Innocent Bystander"
Examples:
Electrolyte abnormalities
Drug toxicity
QT prolongation
Hypoxemia
Severe systemic illness
Characteristics:
Often polymorphic VT
Trigger-driven
Substrate may be reversible
Treating the trigger often eliminates the arrhythmia
Case 1: Scar-Mediated Monomorphic VT
Presentation 68-year-old man, prior anterior MI (EF 25%) ischemic cardiomyopathy presents with wide-complex tachycardia at 168 bpm
Pale and diaphoretic and mild shock physiology
Why Is This VT Until Proven Otherwise?
The old electrophysiology teaching remains true:
A regular wide-complex tachycardia in a patient with structural heart disease is VT until proven otherwise.
Several studies have demonstrated that most wide-complex tachycardias in this population are ventricular in origin.
Clues Favoring VT
Prior MI
Reduced EF
Structural heart disease
Extreme axis deviation
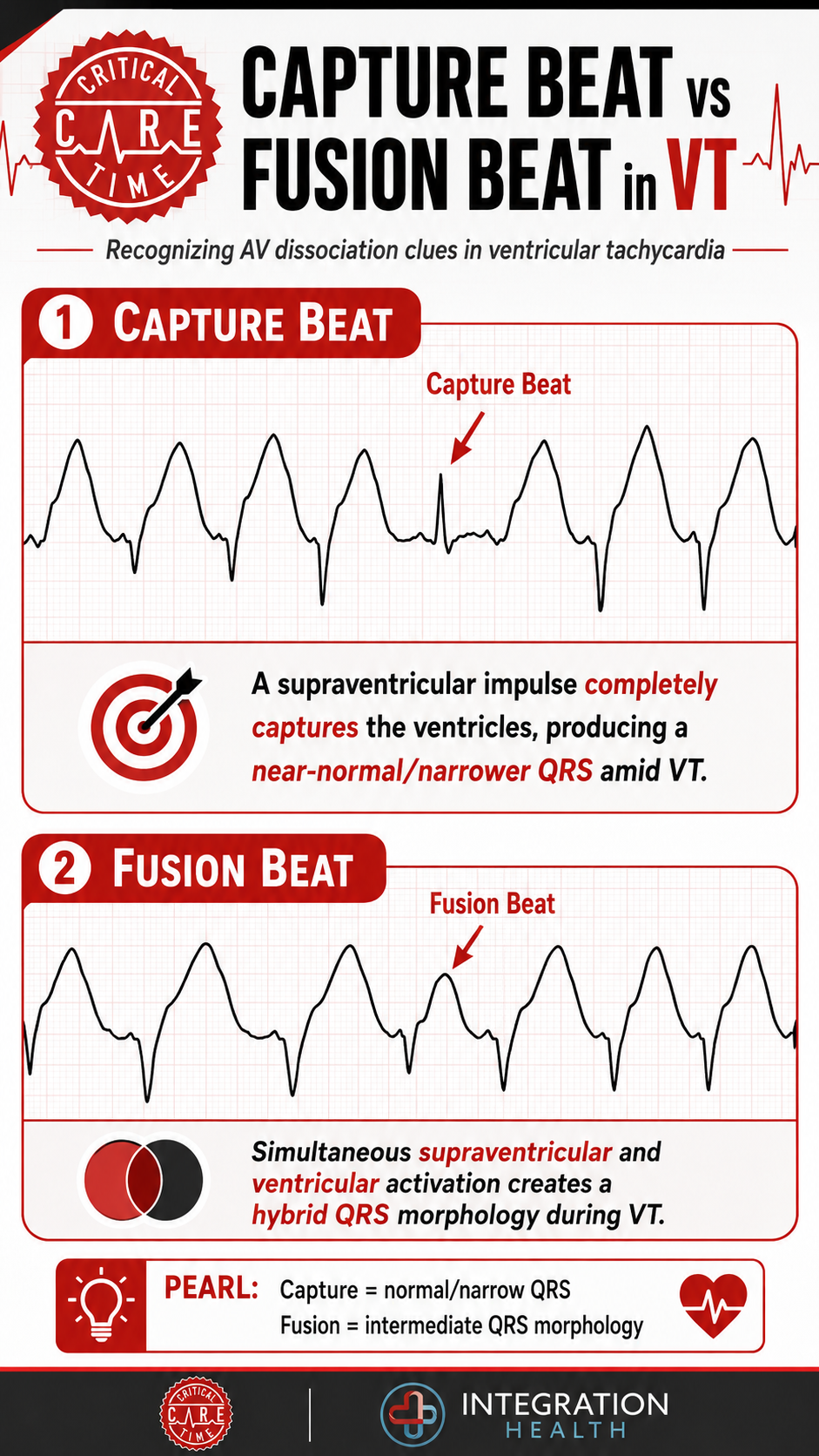
AV dissociation
Capture beats
Fusion beats
Helpful Algorithms
Brugada algorithm
Vereckei algorithm
However:
In the ICU, treatment should not hinge on perfect ECG interpretation.
If the patient is unstable, cardiovert.
Pathophysiology of Scar VT
Following myocardial infarction:
Necrotic myocardium becomes scar
Islands of surviving myocytes remain
Electrical conduction becomes slow and heterogeneous
This creates the ideal conditions for reentry.
The impulse continuously circles around areas of scar tissue:
Slow conduction
Unidirectional block
Reentrant loop
This mechanism explains why monomorphic VT tends to be highly reproducible.
Why Patients Suddenly Crash
Many VT patients initially appear "stable." This can be misleading.
VT reduces cardiac output through several mechanisms:
Loss of AV Synchrony
Loss of atrial kick:
Less LV filling
Reduced preload
Particularly problematic in:
Elderly patients
Diastolic dysfunction
Cardiomyopathy
Reduced Diastolic Filling Time
Higher rates shorten filling time.
Less filling → less stroke volume.
Inefficient Ventricular Contraction
Electrical activation is abnormal.
Mechanical contraction becomes inefficient.
Increased Myocardial Oxygen Demand
The ventricle works harder while receiving less coronary perfusion.
This can worsen ischemia and further destabilize the rhythm.
Practical ICU Treatment Sequence
Step 1: Prepare for Cardioversion
If there is any concern for instability:
Pads on
Defibrillator ready
Vasopressors available
Airway plan prepared & briefed
Do not wait for the blood pressure to completely collapse.
Step 2: Sedation
Patients remember shocks, pain worsens tachycardia and potentially ischemia. Sedation is not optional whenever feasible!
Options include:
Etomidate
Propofol
Dexmedetomidine
Fentanyl adjunctively
An additional benefit: reducing sympathetic activation can help suppress VT.
Step 3: Synchronized Cardioversion
Practical pearls:
Use adequate energy
Wipe away sweat
Ensure pad contact
Consider AP pad placement in obesity or emphysema
Procainamide vs Amiodarone
The PROCAMIO trial compared IV procainamide and IV amiodarone in stable monomorphic VT.
Findings
Procainamide:
More effective termination
Fewer major adverse events
Limitations
Small study
Fragility index = 1
Many intensivists still reach for amiodarone because:
Familiarity
Broad applicability
Ease of administration
Practical Drug Strategy
Dr. Crager's approach:
Shock if unstable
Amiodarone first-line in many ICU patients
Lidocaine particularly attractive in ischemic VT
Escalate early if recurrent
Avoid stacking antiarrhythmics indiscriminately.
Examples:
Procainamide + amiodarone → hypotension risk
Lidocaine + procainamide → neurologic toxicity
Key Takeaway
The biggest mistake is mistaking a temporarily compensated VT patient for a stable VT patient.
If you are escalating vasopressors simply to tolerate VT, the rhythm itself likely needs definitive treatment.
Case 2: Electrical Storm
Presentation:
59-year-old woman with NICM (EF 20%) s/p CRT-D
Presents with cardiogenic shock
Six ICD shocks overnight
What Is Electrical Storm?
Most commonly defined as:
≥3 sustained VT/VF episodes within 24 hours requiring intervention.
Electrical storm represents a self-perpetuating cycle.
The Vicious Cycle
VT causes, Shock, Ischemia, Catecholamine release
These then worsen Electrical instability, Ventricular irritability
Repeated ICD shocks amplify sympathetic activation.
Immediate Trigger Hunt
Ischemia
Acute coronary occlusion remains a major trigger.
Ask:
Is a cath needed?
Is there ongoing infarction?
Obtain a 12-lead ECG after rhythm conversion.
Heart Failure
Worsening congestion (stretch, ischemia, neurohormonal activation) all promote VT.
Electrolytes
Reasonable targets:
K > 4.0–4.5 mEq/L
Mg > 2.0–2.2 mg/dL
Medications
Look for:
Beta agonists
Catecholamines
Drug toxicity
Renal accumulation
Device Issues
ICD interrogation is critical.
Questions:
Appropriate shocks?
Inappropriate shocks?
ATP available?
Reprogramming needed?
Sympathetic Tone Is the Enemy
Perhaps the most important concept in electrical storm:
The sympathetic nervous system fuels VT.
Treating the rhythm while ignoring adrenergic activation is often ineffective.
Four Parallel Treatment Lanes:
1. Antiarrhythmics
Typically Amiodarone or Lidocaine
2. Beta Blockade
One of the most underappreciated therapies.
Benefits:
Suppresses adrenergic stimulation
Reduces recurrent VT
Interrupts the storm cycle
Esmolol is attractive because:
Rapid onset
Rapid offset
Easy titration
3. Sedation
Adequate analgesia and sedation matter.
Options:
Fentanyl
Dexmedetomidine
Deep sedation when necessary
Reducing sympathetic tone can dramatically reduce VT burden.
4. Preserve Perfusion
Consider:
Impella
VA-ECMO
Particularly when recurrent VT is causing cardiogenic shock.
When Drugs Are Failing
Escalate early.
Consult EP early.
Options include:
Catheter Ablation
Definitive treatment for many scar-mediated VTs.
Ablation was superior to escalating antiarrhythmic therapy.
Stellate Ganglion Block
Reduces sympathetic outflow.
Increasingly used for refractory electrical storm.
Key Takeaway
Electrical storm requires simultaneous management of:
Arrhythmia (cardioversion, anti-arrythmiac therapy)
Trigger (sedation, electrolytes, etc)
Sympathetic activation (beta blockers)
Organ perfusion (MCS)
Repeated ICD shocks are not simply evidence that therapy is working. They may be contributing to the disease process.
-
Ortiz M et al. Eur Heart J. 2017. PROCAMIO Trial
Sapp JL et al. NEJM. 2016. VANISH Trial
-
-