#76 ICU Sustainability
This week on Critical Care Time we take a slight departure from our usual content and turn an eye towards sustainability in the ICU. What low-hanging fruit exists in your ICU in the fight against medical waste? Why reach for a nebulizer when HFAs are so much more convenient? We had a great chat with Dr. Stephanie Maximos and Dr. Hari Shankar where we unpack this emerging concept and discuss options to take great care of your patients AND be mindful of waste and excess in your ICU! Listen, learn and let us know what you think!!
Our Guests


INFOGRAPHIC: ICU Sustainability
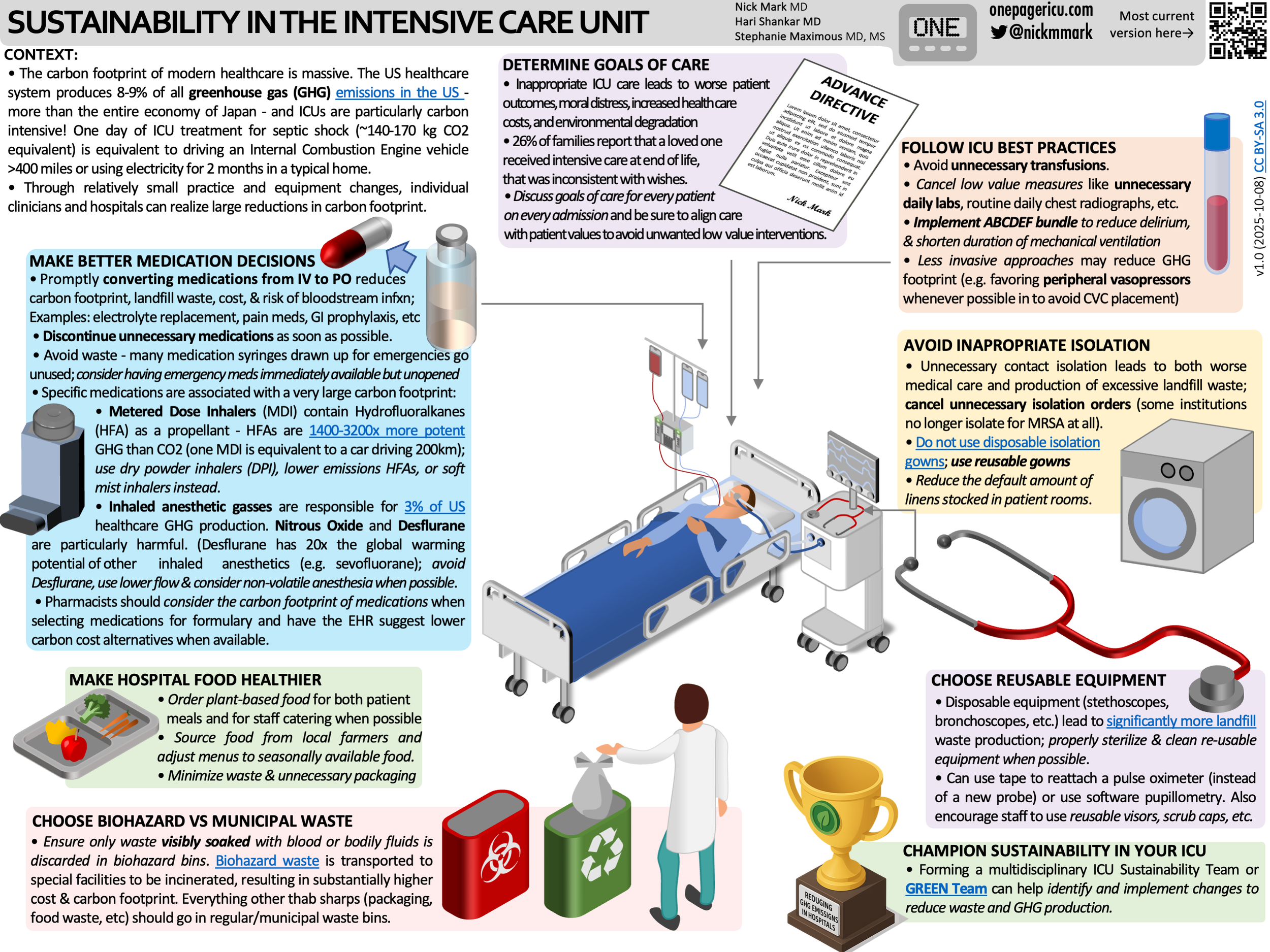
ICU OnePager on Sustainability in the ICU.
What is ICU Sustainability?
Modern intensive care medicine saves lives every day. But it also comes with a significant environmental cost. ICU care is among the most resource-intensive forms of healthcare: high electricity consumption, large volumes of disposable supplies, complex pharmaceutical regimens, energy-hungry devices, and substantial waste generation.
A single day of ICU care for a patient with septic shock may generate roughly 140–170 kg of CO₂-equivalent emissions, approximately the same as:
Driving a gasoline car more than 400 miles
Or powering an average home for nearly two months
And this isn’t a niche issue. The US healthcare system is responsible for approximately 8–9% of total US greenhouse gas emissions. If the American healthcare system were a country, its emissions would exceed those of many industrialized nations, more than the entire economy of Japan by some estimates.
Much of the environmental footprint of ICU care is driven not by necessary treatment, but by inefficiency, waste, redundancy, and low-value practices. Small improvements, multiplied across thousands of patients and ICU days, can produce substantial reductions in waste, emissions, and cost while improving patient care and experience at the same time.
Sustainability in the ICU is not about denying care or rationing life-saving therapies.
Sustainability is high-value, evidence-based critical care.
What can clinicians actually do?
High-value ICU care
Many sustainability interventions are simply good critical care practice.
ABCDEF bundle
The ABCDEF bundle:
reduces ventilator days,
shortens ICU length of stay,
improves delirium outcomes,
and likely lowers environmental impact indirectly by reducing resource utilization.
Goals-of-care discussions
Early alignment with patient goals is one of the highest-value interventions in medicine.
Avoiding non-beneficial ICU care:
prevents suffering,
respects patient preferences,
and reduces unnecessary resource use.
This is not about withholding appropriate treatment. It is about avoiding inappropriate treatment.
Pharmacy
Prefer lower-emission therapies when appropriate
Transition MDIs thoughtfully
Avoid high-impact anesthetic gases when possible
Minimize nitrous oxide and desflurane
IV → PO conversion
Whenever clinically appropriate:
Convert antibiotics
Convert electrolyte replacement
Convert maintenance medications
Oral medications:
reduce packaging,
reduce line access,
reduce nursing workload,
and reduce waste.
Deprescribing
Regular medication review matters.
Stop unnecessary medications
Eliminate duplicate therapies
Avoid “forever ICU meds”
“No MIVF”
Maintenance IV fluids are often continued reflexively despite adequate enteral intake.
Avoiding unnecessary fluids:
reduces plastic waste,
reduces pharmacy burden,
and may improve patient outcomes.
Respiratory care
Lower FiO₂ when possible
Excess oxygen use is common in critical care and may be harmful. It is also very energy intensive to produce oxygen. Routinely
Bronchoscope choice
Disposable bronchoscopes offer convenience and infection-control advantages in some scenarios, but reusable systems may have lower lifecycle emissions depending on institutional workflows.
MDI considerations
Hydrofluoroalkane (HFA) propellants have significant greenhouse impact. Switching to alternative inhalers or nebulizer can substantially reduce carbon footprint.
Reusable equipment
Many disposable items exist largely because of institutional habit. Buying reusable items can incur significant reductions in waste and are often more cost effective in the long run. Examples:
Reusable stethoscopes
Reusable gowns
Durable equipment instead of single-use tools
Waste and isolation
Avoid unnecessary disposal
Not every item needs replacement immediately. Simple examples:
Reattaching pulse oximeter probes with tape
Reusing intact positioning devices
Avoiding opening supplies “just in case”
Biohazard vs regular trash
A surprisingly large proportion of “biohazard” waste does not actually require biohazard processing. Biohazard (“red bag”) waste is driven to a special facility and incinerates, generating substantially larger carbon footprint than other waste. (also much more expensive)
Proper waste segregation can substantially reduce waste streams.
Biohazard trash is necessary for materials saturated in blood/waste.
Regular domestic waste or recycling is usually sufficient for items with dried spots of blood, or gloves/bandages that are not dripping or caked.
Many items used in the ICU can be recycled:
Many medical device manufacturers (like Stryker, Medline, and Vanguard) sponsor take-back programs to reprocess high-value, single-use items so they can be clinically sterilized and reused
Recycling is possible with many ICU items such plastic tube feed containers, glass medication vials, and other plastics/polymers (uncontaminated basins, etc)
Contact isolation
Isolation precautions are important when truly indicated, but are often applied incorrectly and continued unnecessarily.
Excess isolation:
increases waste,
increases PPE use,
likely worsens patient care
and can contribute to delirium and reduced clinician interaction.
Solutions:
Promptly discontinue when cleared.
Discuss criteria for isolation (e.g. does MRSA really require contact isolation?)
Consdier reusable gowns; this may reduce waste substantially.
Food and catering
Hospital food systems also contribute significantly to healthcare emissions.
Potential strategies:
More locally sourced food
More plant-forward options
Reducing food waste
Even conference catering and departmental events are opportunities to think intentionally about sustainability.
ICU energy use
Simple operational changes matter:
Turn off unnecessary lights at night
Reduce unnecessary cooling
Shut equipment off instead of leaving it in standby mode
These changes may also improve:
sleep,
delirium prevention,
and patient comfort.
ICU “Code Green” teams
Sustainability works best as a multidisciplinary effort. Potential participants:
Nursing
Pharmacy
Respiratory therapy
Environmental services (EVS)
Physicians
Hospital operations
Potential projects:
Quality metrics (e.g. ABCDEF bundle adherence, early extubation, etc)
Formulary changes (e.g. change MDIs to nebulizers)
Order-set optimization (e.g. electrolyte replacement PO if possible)
Equipment standardization (e.g. procedure trays that produce less waste)
Reusable equipment programs (e.g. use of disposable vs reusable bronchoscopes, reusable pulse oximeters, software pupillometers, etc)
Education campaigns (e.g. what has to be put into biohazard trash)
Waste audits (e.g. how many bags of biohazard trash produced per week after an education campaign)
Sustainability dashboards and infographics (bags of trash, number of MDIs used, etc)
Small operational changes can scale quickly across an ICU, a hospital system, or an entire region resulting in significant reductions in carbon footprint.
Interactive: How GREEN is your ICU?
Try out this interactive calculator here. You can estimate what the impact of different interventions could be. As always the code is available and the app is open-source.
Additional Resources
Health Care Without Harm
The Shift Project — Healthcare Sustainability Resources