#75 The APRV Debate
On this week’s episode, Cyrus and Nick host a spirited discussion with Drs. Rory Spiegel and Max Hockstein where we debate the merits of Airway Pressure Release Ventilation (APRV). What's the rationale for this? When is it appropriate? IS it appropriate… or is it witchcraft? Is it physiologically foolish or a perfectly logical option for hypoxemic respiratory failure? Good for all comer, good for a subset or does it belong with the vials of succinylcholine and DL blades? We may not have all the answers but on this episode we do our best to explore this ventilator mode and help you decide whether the juice is worth the squeeze! Check us out and let us know YOUR feelings while leaving us a review!
Our Guests

What is APRV?
A pressure-controlled, time-cycled mode of ventilation that maintains a high continuous airway pressure Phigh for a prolonged period Thigh with brief, intermittent releases to a lower pressure Plow for a short time
Evidence is mixed: No consistent mortality benefit in randomized trials compared with lung-protective ventilation.
Hard to standardize/teach: Steep learning curve; settings (especially Tlow) are somewhate nuanced.
Monitoring challenges: Tidal volumes are variable and not directly set → risk of unrecognized volutrauma.
APRV isn’t new - it’s old!
Airway pressure release ventilation (APRV) was first described in 1987 and defined as continuous positive airway pressure (CPAP) with a brief release while allowing the patient to spontaneously breathe throughout the respiratory cycle
The 30 year history of APRV is well summarized here.
What do the studies say?
The first RCT was done in 2004 (n=58, compared to SIMV) and found no advantage. It was stopped early for futility.
This same group (varpula et al) did another RCT (n=45) combining APRV with prone positioning and found a small benefit when APRV was combined with proning, compared
Another RCT was published in 2010 (n=63, also compared to SIMV), focusing just on trauma patients. It found no advantage with APRV
Another RCT by Song et al in 2016 (n=26) was also negative.
Largest RCT by Zhou et al in 2017 randomized n=138 patients at a single site: “critical care medicine unit (ICU) of the West China Hospital of Sichuan University”
This is the only RCT to find any benefit in terms of hard endpoints - this found an almost impossible to believe difference in ventilator free days: 19 interquartile range (IQR) 8-22] vs. 2 (IQR 0-15) but no significant difference in mortality (19.7% in the APRV group versus 34.3% with LPV).
Significant limitations of the study included a higher rate of comorbid conditions in the control group, internal inconsistencies, and the fact that the groups were not balanced (vasopressor use).
Notably they used a lot more recruitment maneuvers, oscillatory ventilation, and paralytics in the LTV group. Recruitment maneuvers and oscillator ventilation are both associated with increased complications and mortality.
In 2018, Hirshberg et al did a 4 ICU RCT of APRV vs LTV-APRV vs conventional LTV. Unfortunately at n=53 the trial was under-enrolled and stopped early due to trouble recruiting.
In 2021, Estabara et al did an RCT of APRV in COViD patients (n=45). They found no benefit with 78% mortality in airway pressure release ventilation vs 60% in low tidal volume; p = 0.07).
Also in 2021, Kucuk et al did an RCT of n=65 patients who were at risk for ARDS and were randomized to SIMV + PS vs APRV.
Found no difference in mortality.
Also found no difference in the sedation between groups!
In 2025, Zou et al did a small (n=40) trial of APRV vs LTV published in CHEST,
Zhou et al are apparently planning a n=840 multi-center RCT at multiple sites in China. (this is the same group that did the other positive trial)
Data on APRV in COVID ain’t great
One Observational trialfound increased mortality
Another trial found no difference.
Synthesis
However APRV does NOT consistently improve survival
Almost all trials have been negative for hard endpoints. More larger trials are ongoing
Proven benefits are physiologic, not clearly patient-centered
Safe only when protocolized and well understood; don’t be the only person in your institution who does it!
“The safest mode is the one that everyone understands”
Conventional lung-protective ventilation remains the standard
Diffusion of Innovation
With any innovation there are a small number of people who use it first: innovators. This is followed by the early adopters and early majority.
The late majority are the people who are slow to embrace the innovation. Laggards are the people who refuse to accept widely accepted practices, years after others have embraced them.
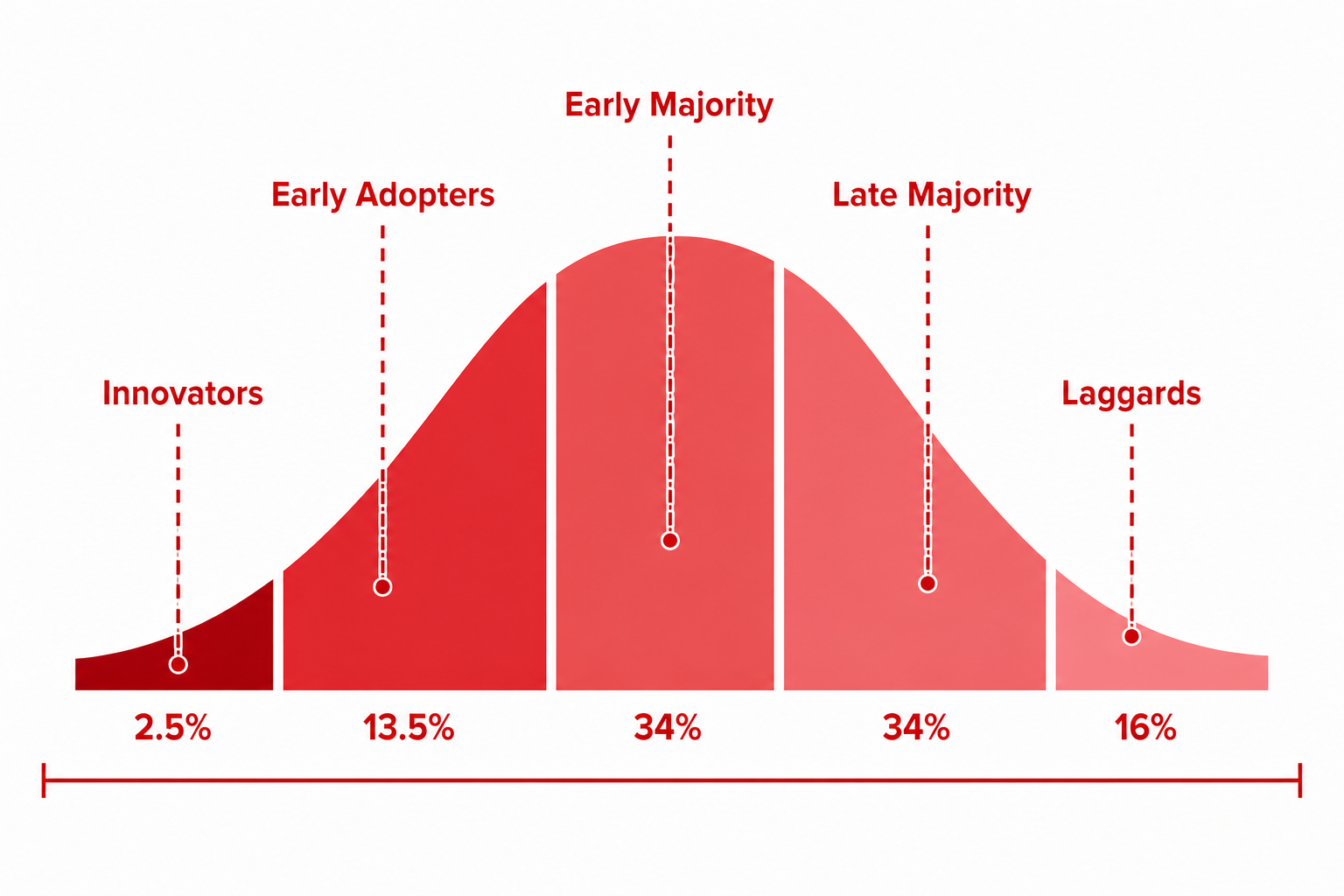
- APRV has been around for 30 years but its use remains limited. Who are the early adopters and who are the laggards? What do you think?
What do you think?
Summary:
Pros:
Improved oxygenation in some patients.
Less sedation/paralysis (if spontaneous breathing tolerated).
Potential hemodynamic benefits vs deep sedation/controlled modes.
May reduce ventilator-induced lung injury via better recruitment (theoretical/physiologic).
Cons:
Variable tidal volumes → potential for lung overdistension.
CO₂ clearance can be tricky (depends on release phase and patient effort).
Requires expertise; easy to mis-set (e.g., T<sub>low</sub> too long → derecruitment).
No clear outcome superiority over standard low tidal volume ventilation.
Can be uncomfortable or dys-synchronous in some patients.
Bottom line:
APRV is a physiologically appealing but operator-dependent mode. It can work well in experienced hands for selected patients, but it hasn’t clearly beaten conventional lung-protective ventilation—which keeps it in the “controversial but useful” category rather than standard of care. Stay tuned for ongoing RCTs.
Learn more here:
- Max and Rory’s field guide to using APRV(must read reference)
- Read Rory’s excellent article ‘The Things we Carried” (highly recommended)