#72 ICU Toxicology
On this week, Cyrus & Nick are joined again by intensivist extraordinaire, Dr. Adam Mora, for a long overdue episode on ICU Toxicology! Together, the three of us embark on a case-based journey covering some of the more common ICU toxidromes as well as some of the more unusual, but can't-miss diagnoses. This is a bit of a longer one but it's super high-yield and very practical for anyone who is studying for their boards and/or participating in the care of the critically ill! Thanks to our tag-team of sponsors for this episode: The Difficult Airway Course: Critical Care and our newest sponsor, Integration Health!
Overview
In this high-yield, case-based episode, we take a tour de toxidromes with returning guest Dr. Adam Mora (UT Southwestern, Intensivist with expertise in OB and Transgender Critical Care).
This is not a comprehensive tox textbook—but rather a practical ICU-focused framework to rapidly recognize and manage some of the most common (and deadly) toxicologic emergencies.
Guest:

Adan (Adam) Mora Jr., M.D.,
Associate Professor in the Department of Internal Medicine at UT Southwestern Medical Center.
He specializes in the management of critically ill pregnant patients and critically ill transgender patients, resuscitation execution, and end-of-life care in the intensive care unit (ICU).
The ICU Approach to Toxicology
Across all cases, a few recurring themes:
Recognize patterns (toxidromes) quickly
Stabilize airway, breathing, circulation first
Don’t wait for confirmatory labs to start treatment
For any toxicology emergency consider:(Nick’s “5 what’s and a why”)
What drug?
What dose?
What route?
What time?
What else?
Why?
Remember that co-ingestions can muddle typical toxidrome patterns (e.g. co-ingestion of a stimulant and an anticholinergic)
Opioid Toxicity
Presentation
Found unresponsive in bathroom
Pinpoint pupils, hypoventilation
Transient response to naloxone → re-sedation
Key Data
RR 6, SpO₂ 82%
ABG: pH 7.19 / CO₂ 78 → severe hypercapnic respiratory failure
Pupils: 1 mm
Diagnosis: Opioid toxidrome
CNS depression
Respiratory depression
Miosis (but may be absent with co-ingestion)
Teaching points:
Pupils matter—but aren’t perfect
Pinpoint pupils = classic
BUT:
Co-ingestions → normal pupils
Tramadol → atypical
Naloxone strategy
Goal: restore ventilation, NOT full wakefulness
Target: RR ≥ 10–12
Avoid overshooting → withdrawal
Escalation: Repeat boluses → then infusion
Infusion = typically ~2/3 of effective “wake-up dose” per hour
Avoid precipitated withdrawal
Use 0.04 mg incremental dosing
High-dose naloxone will cause vomiting, agitation, aspiration
Critical co-ingestions to consider
Xylazine (“Tranq”) → 🔥 HIGH-YIELD
Veterinary Alpha-2 agonist
“Temu Precedex”
Effects:
Profound sedation
Bradycardia
NO response to naloxone
Clues:
Necrotic skin ulcers → infection risk
Clonidine
Similar physiology
May need pressors (epi/norepi)
Intubation considerations
If intubated: Continue opioid-based sedation
Don’t “reverse then abandon”—you’re treating physiology
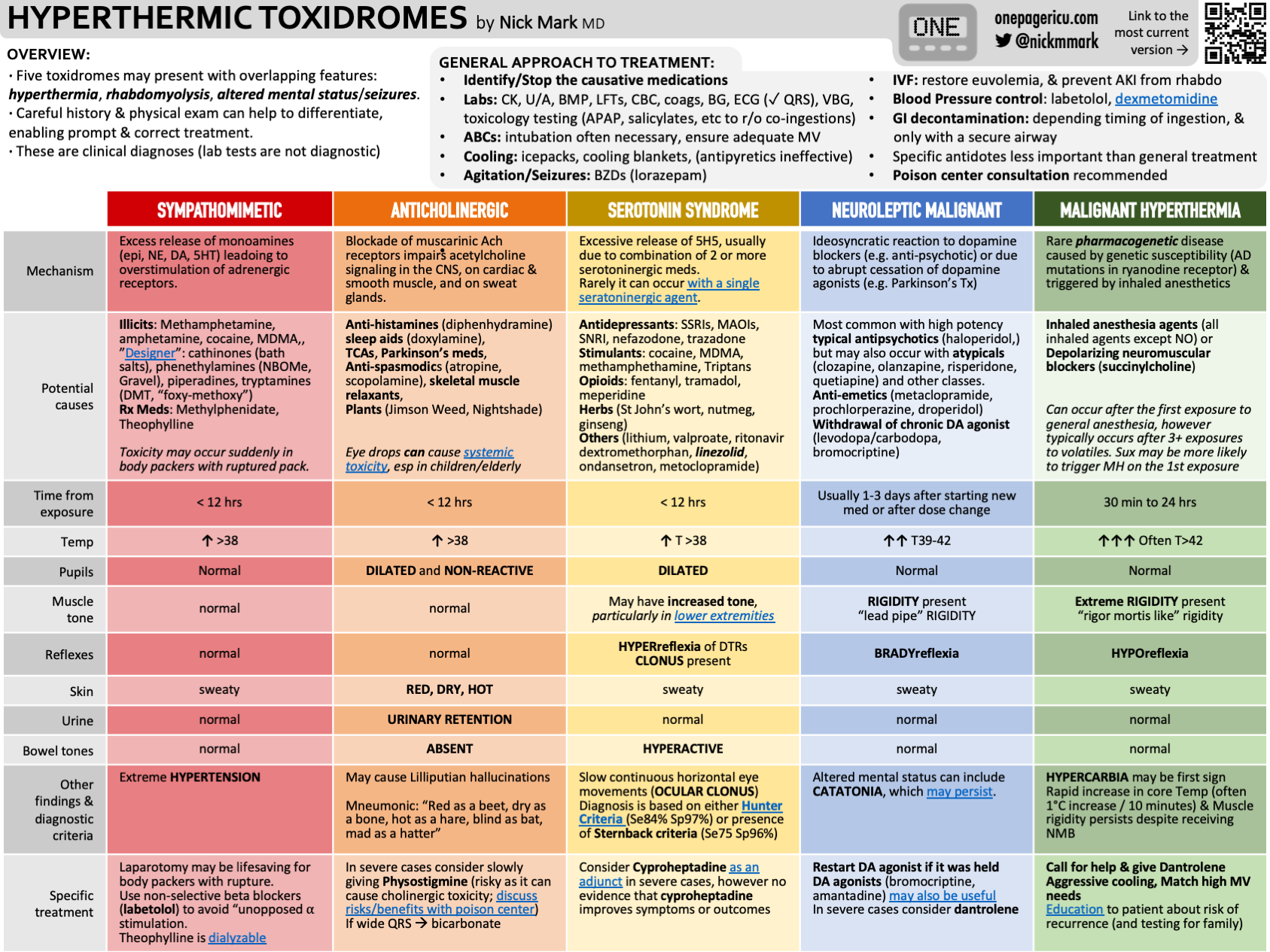
Serotonin Syndrome
“The agitation + clonus combo”
Presentation
SSRI + migraine medication
Agitation, hyperthermia, tremor
Key Data
T 39.2°C
Clonus (ankle + ocular)
CK 2400
Diagnosis: Serotonin syndrome
Hunter Criteria (high yield)
Clonus + agitation = diagnosis
Differentiating “Hot & Bothered” Toxidromes
Management
🚫 Step 1: STOP offending agents
💊 Sedation
Benzodiazepines = first line
DO NOT give antipsychotics
🌡️ Temperature strategy
Temp Treatment
<38.5 BZDs + passive cooling
38.5–40 Aggressive cooling
>40 INTUBATE + PARALYZE STAT
⚠️ Avoid succinylcholine (rhabdo/hyperK risk)
Toxic Alcohols
“AGMA + blurry vision”
Clues about particular alcohols
Methanol —> Vision (“snowstorm”)
Ethylene glycol —> AKI + crystals
Isopropanol —> Osm gap only
Osmolar Gap
Elevated early
AG rises later
Treatment
Fomepizole → DO NOT WAIT
Vitamins
Folate
Thiamine
Pyridoxine
Dialysis
Methanol >50
Severe acidosis or symptoms
Pitfalls
False lactate elevation (POC assays)
Delayed AG → don’t anchor
Intubation danger
Severe acidosis → maintain compensation
Avoid dropping minute ventilation
Anion Gap and Osmolar Gap Calculator
Key Takeaways
Recognize patterns, not just numbers
Treat physiology first
Don’t wait for confirmatory tests when suspicion is high
Avoid causing harm with the wrong “fix”
Always consider co-ingestions
This Episode was Proudly Sponsored By:
