#73 Diabetic Ketoacidosis

On this week's episode of Critical Care Time, Cyrus & Nick go all-in on DKA and spend a little time talking about alcoholic and starvation ketosis too! In this jam-packed, clinically robust episode, the guys discuss the importance and pathophysiology of DKA before discussing all things treatment. After listening to this - and perusing the show notes - you'll be a DKA master! Check it out and let us know what you think. Special thanks to Integration Health and The Difficult Airway Course: Critical Care for supporting the production of this episode!
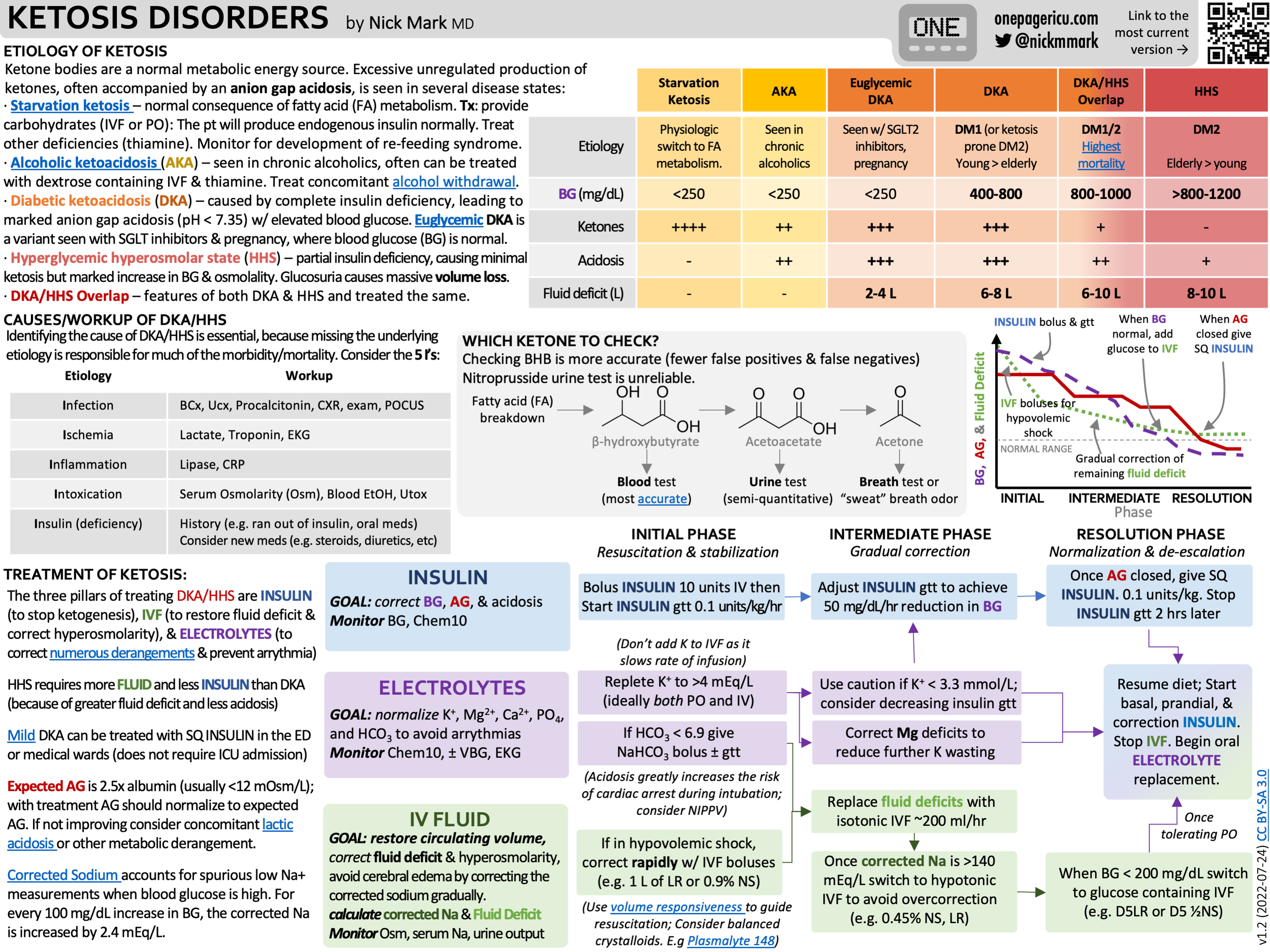
ICU OnePager on Ketosis Disorders
Morbidity and mortality in DKA largely results from two errors:
Failure to identify/treat the cause of DKA
Failure to correct metabolic derangements
Use the “Five I’s” mneumonic to identify causes/precipitants:
Infection
Ischemia
Inflammation
Intoxication
Insulin deficiency
Consider that not all ketosis is DKA. Other etiologies include:
Starvation ketosis - a physiologic switch to ketone metabolism. Treatment: feeding, watch for re-feeding syndrome.
Alcoholic ketoacidosis (AKA) - treat concomitant alcohol withdrawal.
Euglycemic DKA - DKA without hyperglycemia. Can be seen in pregnancy or with SGLT2 inhibits
Hyperglycemic Hyperosmolar State (HHS) - hyperglycemia without ketogenesis. Typically higher glucose and more volume losses.
DKA/HHS Overlap - HHS that subsequently develops ketogenesis, displaying features of both. Highest mortality.
Diagnosis of DKA -
Confirm the presence of ketones:
Blood: detects beta-hydroxybutyrate (most sensitive and specific test)
Urine dipstick: detects acetoacetate
Breath: acetone
Measure anion gap, blood glucose, pH, and electrolytes
The Three Pillars of Treatment of DKA
Insulin - the goal is to suppress ketogenesis, correcting AG, BG, and acidosis
Bolus followed by a continuous infusion
Electrolytes - the goal is to restore losses, maintaining appropriate levels of potassium, magnesium, and phosphate
Aggressive replacement, typically parenterally and enterally.
Remember that magnesium deficiency prevents correction of concomitant potassium deficiency.
Fluids - the goal is to restore euvolemia
Bolus followed by infusion.
LR is a common choice. Add glucose (such as D5LR) once the BG is < 250 if the anion gap remains open.
Treatment has three phases
Initiation - boluses of insulin, fluid
Correction - gradual controlled correction with frequent monitoring of labs
Resolution - transition to SQ insulin, resumption of diet, etc
Anion Gap and Osmolar Gap Calculator
This Episode was proudly sponsored by:
