#70 Right Heart Failure with Dr Matt Siuba
Buckle up because on this week's episode of Critical Care Time we are treated to a master class on Right Heart Failure with world-class educator Dr. Matt Siuba. We are taking a deep dive on diagnosis, management and of course, sharing our love for the PAC! Make sure you clear your schedule and take notes for this one because as far as we are concerned, this is required listening for anyone who cares for the critically ill!

Dr. Matt Siuba
“The RV is the ventricle of the downtrodden”
Part 1 — Why the Right Ventricle Is the “People’s Ventricle”
“The People’s Ventricle” is a nod to A People's History of the United States by Howard Zinn — and yes, a subtle wink to Good Will Hunting.
The right ventricle (RV) is the overlooked chamber. It doesn’t get the glamour of the LV. It runs low pressures. It operates quietly. But when it fails, it can bring down the entire circulation with astonishing rapidity.
Key physiological differences between RV and LV:
Pressure: The RV/pulmonary circulation is a low pressure circuit, high compliance circuit (in contrast to the LV)
The RV wall normally < 5 mm; it cannot acutely generate high pressure —> the acutely injured RV rarely sustains RVSP > 60 mmHg
Contractility: The RV has 1/3 to 1/5 the contractility of the LV → thus the RV has less physiological reserve
Fiber orientation: 80% of the RV cardiac output is via lengthwise contraction (in contrast to primarily concentric contraction in the RV)
Perfusion: The RCA perfuses the RV in systole and diastole (unlike the LV which is perfused only in diastole but multiple coronary vessels); RV perfusion is heavily dependent upon MAP and has little redundancy.
Understanding the RV Death Spiral:
Increased afterload → RV dilation → septal shift → ↓ LV preload → worsening shock
RV dilates to maintain stroke volume (Frank–Starling adaptation)
Stretch is initially adaptive, however Progressive dilation is maladaptive
Septal bowing causes intraventricular dependence, reducing LV stroke volume.
Impaired LV filling → systemic hypotension → worsened RV ischemia
This is why RV dysfunction is uniquely catastrophic.
What Causes RV Failure in the ICU?
Assume RV dysfunction until proven otherwise in:
Pulmonary Vascular Stressors
Acute PE
ARDS
Hypoxemia
Hypercapnia
Acidemia
Sepsis
Pulmonary hypertension (PH)
Definition update: Mean PAP > 20 mmHg defines PH (2022 ESC/ERS Guidelines)
Ischemic Causes
Isolated RV MI (RCA territory)
Larger infarcts involving the inferior wall (RV often neglected, initially)
PH Triggers in ICU
Hypoxia
Hypercapnia
Sepsis
Tachyarrhythmias
PE
RV and Ventilator Interactions
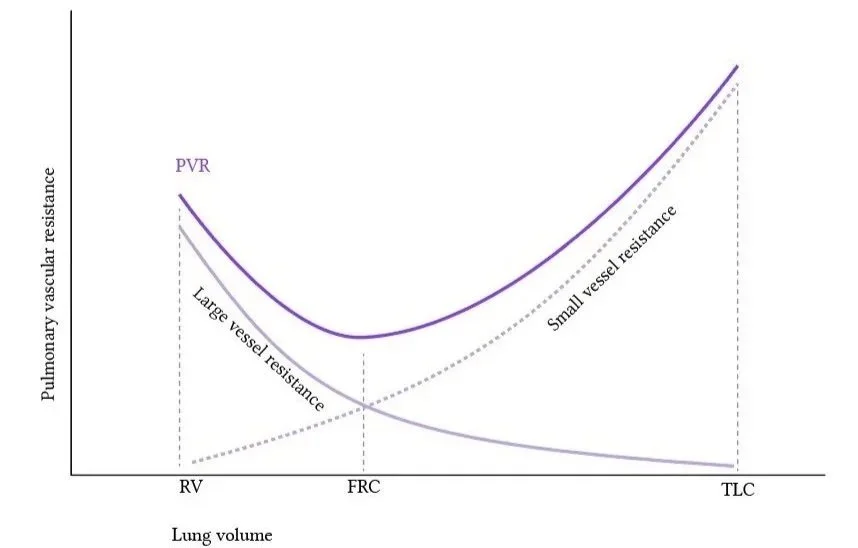
U-shaped relationship between Pulmonary Vascular Resistance (PVR) and Tidal Volume (TV); note the rising PRV with lung volumes either above or below FRC.
Positive pressure ventilation increases RV afterload by:
Increasing transpulmonary pressure
Compressing pulmonary capillaries
Increasing PVR
PVR vs lung volume is U-shaped.
Too little PEEP → atelectasis → ↑ PVR
Too much PEEP → overdistension → ↑ PVR
Practical Targets
Driving pressure < 15 cmH₂O (ideally < 12–13)
Avoid severe hypercapnia (can increase PVR)
In obesity: plateau pressure may be higher but driving pressure still safe
Hypercapnia + rising dead space may signal overdistension.
Part 2 — Monitoring the RV
Two Core Questions:
1. How invasive?
2. How repeatable?
Least invasive → Most invasive:
Transthoracic Echo (TTE)
Tranesophageal Echo (TEE)
Central Venous Pressure (CVP)
Pulmonary Artery Catheter (PAC)
Bedside Echocardiogram for assessing RV size and function
1. Size (Apical 4-chamber)
Normal LV:RV ≈ 2:1
RV = LV → dilated
RV > LV → severely dilated
2. Squeeze
TAPSE normal > 1.7 cm (often simplified > 2 cm)
RV fractional area change
Tissue Doppler S’
3. Septal Kinetics
Flattened septum in systole → pressure overload
Flattened septum in diastole → volume overload
When Is a PAC Helpful?
Unselected ICU patients do NOT benefit from routine use of a PAC (PAC-MAN trial) however it can be immensely useful in the right patient.
Ask:
How uncertain am I?
How sick is the patient?
Will the data change management?
But:
“A PAC is useless if you only look at one number.”
Use it as a Starling curve generator.
Key Metrics
CO/CI (must use!)
PVR = (Mean PAP – PCWP) / CO
Distinguish:
Pre-capillary PH → PVR ≥ 2 Wood units
Post-capillary PH → PCWP elevated
Thermodilution remains reasonably accurate even with TR
Continuous vs Intermittent CO
CCO PAC allows trending
Direct Fick = gold standard but impractical in ICU
Indirect Fick assumes estimated VO₂ which is often wrong.
Role of the pulmonary artery catheter (PAC) in 2026:

“I gottah numba! How ‘bout them apples?”
“Zentensivism” vs ICU Nihilism
Zentensivism is:
Minimally invasive
Maximally attentive
Uses no crystals except the ultrasound ones
Elevates the humanity of the patient
Never involves placing devices without purpose
Thoughtfully choosing interventions based on your patients goals and physiology is the essence of Zentensivism. It requires a deep understanding of the literature and the reason you are performing an intervention.
In contracts, ICU Nihilism is a misunderstanding of physiology and the evidence. It often manifests with blanket statements like:
“PACs don’t improve survival” (PAC-MAN)
“Art lines aren’t beneficial in sepsis” (EVERDAC)
“No one should be checking CVP and ScvO2 anymore”
How does a Zentensivist respond to ICU Nihilism:
PAC-MAN showed no survival benefit in unselected patients, mostly with sepsis and when placed without ultrasound. That doesn’t inform contemporary placement in carefully selected patients with RV failure.
EVERDAC showed routine placement of art lines in all ICU patients on vasopressors didn’t improve mortality. It was underpowered. Most ICU patients on low dose vasopressors don’t need an art line.
CVP has been demonstrated not to be an effective resusciation target in septic shock. It can provide useful information when evaluating other etiologies of shock such as RV failure.It means: use thoughtfully.
Be an Zentensivist not an ICU Nihilist
We discuss several of these trials - and their limitations - at greater length in other episodes:
Part 3 — Managing RV Failure
Therapeutic schema:
Lower afterload
Optimize preload
Support contractility
Maintain oxygenation
Support systemic perfusion
Afterload: “The Most Energetically Favorable Target”
Lowering PVR is “free cardiac output.”
Oxygen
Even 6 L/min NC vs room air can improve RV function in PH patients (Rich et al., CHEST 1982).
Avoid:
Hypoxemia
Hypercapnia
Acidemia
Pulmonary Vasodilators
Inhaled nitric oxide (iNO)
iNO → U-shaped PVR response
Inhaled epoprostenol (EPO)
EPO → more linear
Both:
Delivered via ventilator or HFNC
Reduce PVR
Must reassess: CO ↑, mean PAP ↓
Be cautious in the presence of shunt physiology.
Preload: “The RV Is Preload Intolerant”
When you meet a sick RV, it’s usually volume overloaded.
Goals:
Normalize geometry
Reduce septal shift
Clues:
CVP waveform without respiratory variation → volume overloaded
Large Y descents → volume overload
Portal vein pulsatility and VExUS can help.
Avoid BNP to manage critically ill RV failure.
Monitor perfusion: B-U-S
Brain —> are they mentating?
Urine —> are they peeing?
Skin —> cap refill?
Contractility
After optimizing preload and afterload, consider enhancing RV contractility
Inotropes
Dobutamine
Rapid onset/offset
Can lower SVR
Milrinone
Prominent pulmonary vasodilator effect
Longer half-life, especially in renal failure
More systemic hypotension
Epinephrine
Strong inotropy
May raise lactate
DORAME study (n=16 isolated RV failure) suggests dobutamine improves hemodynamics (Haddad et al., Crit Care Med 2009).
Vasopressors: Choose Carefully
Goal:
Maintain systemic pressure > RV systolic pressure
Preserve RCA perfusion
Preferred
Vasopressin
Norepinephrine
Physiologically appealing: Angiotensin II (limited data)
Avoid: Phenylephrine (↑ PVR)
Always consider:
MAP target relative to RVSP
Renal perfusion pressure = MAP – CVP
Mechanical Circulatory Support
Consider when still failing despite:
Afterload optimized
Preload corrected
Inotrope initiated
MCS options in RV failure:
VA-ECMO
RVAD
RV Impella (e.g., Impella RP)
Device choice depends on:
Isolated RV failure?
Biventricular failure?
Transplant candidate?
High-Yield Takeaways
RV failure kills by geometry and perfusion collapse.
Ventilators can worsen RV afterload — lung volume matters.
Lower afterload first. It’s free cardiac output.
The RV is not preload dependent. It is preload intolerant.
Use PAC thoughtfully — not nihilistically.
Maintain systemic pressure above RV systolic pressure.
Optimize oxygenation and avoid hypercapnia.
Sponsored by The Difficult Airway Course: Critical Care
