#80 B2B Arterial Lines

Welcome to Season 4 of Critical Care Time! We are excited to be back for another year of exciting content and what better way to kick things off than with a brand new series! This year we're piloting our Back to Basics series where we will do deep dives on fundamental skills, tests, tools and so much more in the ICU. First up is Back to Basics: All Things Art Lines. On this inaugural episode we discuss why arterial blood pressure monitoring is so important in the ICU, how the place these lines, how to interpret the waveforms and cover a bunch of tips and tricks that you can tuck away for your next A-Line in the ICU! Let us know what you think: Send us a message on socials, drop us a comment or reach out via email!
Arterial catheters are among the most useful monitoring tools in critical care. They provide continuous beat-to-beat blood pressure monitoring, facilitate frequent arterial blood gas sampling, allow advanced waveform analysis, and enable several physiologic measurements that are otherwise difficult or impossible to obtain.
Why Place an Arterial Line?
Arterial lines are most useful when continuous blood pressure monitoring provides information that intermittent cuff measurements cannot.
Common indications:
• Hemodynamic instability requiring beat-to-beat blood pressure monitoring
• Shock states requiring vasopressors or rapidly titrated vasoactive medications
• Situations where non-invasive blood pressure measurements are unreliable
• Cardiac patients requiring continuous hemodynamic assessment
• Severe respiratory failure requiring frequent arterial blood gas analysis
• Severe anemia where minimizing phlebotomy waste becomes important
• VA-ECMO patients, particularly with right radial monitoring to detect differential hypoxemia ("north-south syndrome")
• Cardiac arrest, where arterial pressure monitoring can guide CPR quality and identify ROSC rapidly
The major benefit is not simply obtaining more numbers. The benefit comes from acquiring accurate physiologic information continuously and acting upon it in real time.
POCUS-Guided Placement: The Modern Standard
The era of blind arterial cannulation should be considered over. Modern guidelines strongly recommend ultrasound guidance for arterial cannulation.
The 2025 American Society of Echocardiography (ASE) Guidelines on Ultrasound-Guided Vascular Cannulation recommend ultrasound guidance for arterial access because it improves first-pass success, reduces the number of attempts, and decreases complications.
Practical recommendations:
• Use ultrasound every time
• Scan both sides before choosing a vessel
• Compare radial and ulnar arteries
• Prefer the non-dominant extremity when feasible
• High-dose vasopressors do not automatically preclude radial artery cannulation
Typical procedure:
Ultrasound vessel assessment
Sterile preparation and draping
Local anesthesia with lidocaine
Needle entry under ultrasound visualization
Wire advancement
Confirmation of wire position (bullseye sign)
Catheter advancement
Connection to pressure tubing
Securement and dressing placement
Deliberately Back-walling vessels? Nope
A controversial topic is the deliberate back-wall puncture technique. Historically, some operators intentionally traversed both walls of the artery and then withdrew until blood return was achieved. This approach originated in the pre-ultrasound era. With modern ultrasound guidance, intentionally creating a second arterial puncture likely provides little benefit while increasing hematoma risk, particularly in thrombocytopenic patients and those receiving antiplatelet or anticoagulant therapy.
Securement: Suture or StatLock? BOTH
Dislodgement is not a minor inconvenience. Particularly, in brachial, axillary, and femoral locations, accidental removal can result in substantial hemorrhage, potentially threatening life of limb.
Many anesthesiologists favor adhesive securement devices alone because operative patients remain relatively immobile. ICU patients are different. Agitation, diaphoresis, frequent repositioning, and prolonged dwell times increase dislodgement risk. Suturing is highly recommended for ICU arterial lines.
Limited data compares adhesive vs sutures, but our recommendation is to do BOTH together.
Complications of Arterial Lines
Although generally safe, arterial lines are not benign devices.
Infection
Catheter-related bloodstream infection rates may approach those seen with central venous catheters, particularly for femoral arterial catheters. Infection risk increases with dwell time, emphasizing the importance of daily reassessment and prompt removal when monitoring is no longer required.
Bleeding and Hematoma
Hematoma formation remains the most common complication. Older studies reported rates approaching 14%, though contemporary ultrasound-guided practice likely lowers this substantially. Severe bleeding complications remain uncommon but can be devastating.
Compartment Syndrome
Rare but limb-threatening. Most evidence comes from radial catheterization literature, where incidence appears to be approximately 0.02%.
Vascular Occlusion
Transient arterial occlusion is relatively common after radial cannulation. Permanent clinically significant ischemia is very rare, estimated around 0.09% in some studies.
Nerve Injury
Uncommon but reported. Potential manifestations include neuropathy and complex regional pain syndrome.
Exsanguination
Perhaps the most underappreciated complication. Arterial lines disconnecting from tubing systems can result in life-threatening hemorrhage. Arterial line alarms should never be disabled.
Choosing an Arterial Line Site
Radial Artery
The default choice for most patients.
Advantages:
• Easy compression
• Lowest consequence of bleeding
• Familiar anatomy
• Excellent nursing accessibility
• Lower infection risk than femoral access
Disadvantages:
• Smaller vessel
• Potential waveform distortion during severe vasoconstriction
• Radial artery occlusion
• Possible underestimation of central pressure in extreme shock states
Most clinicians can safely place more than 90% of arterial lines in the radial artery.
Ulnar Artery
An underutilized alternative to radial access. Historically, in the pre-ultrasound era, radial was preferred because it was easier to palpate. (This is no longer true. See Nick’s blog for a longer discussion.) In approximately 60% of people the ulnar artery is larger than the radial, making ulnar potentially superior.
Advantages:
• Similar location and technique to radial access
• Often larger than expected
• Preserves radial artery
Disadvantages:
• Less operator familiarity
• Smaller evidence base
• Historical concerns regarding hand ischemia (never attempt ulnar after a failed radial due to concerns about compromising hand circulation)
ASE guidelines recognize the ulnar artery as a reasonable alternative access site.
Brachial Artery
Advantages:
• Larger target vessel
• Less susceptible to vasoconstriction
• Closer approximation of central pressure
Disadvantages:
• More difficult compression
• Proximity to median nerve
• Potentially more serious ischemic complications
Typically reserved for situations where wrist access is unavailable.
Axillary Artery
Advantages:
• Large vessel
• Central-like pressure measurements
• Useful when upper extremity distal vessels are unavailable
Disadvantages:
• More technically demanding
• Bleeding harder to control
• Brachial plexus proximity
Published series demonstrate excellent success rates but somewhat higher complication rates than radial access.
Common Femoral Artery
Advantages:
• Large target
• Excellent waveform quality
• Reliable access during severe shock, hypothermia, or CPR
• Lowest failure rates
• Useful when VA-ECMO may be required
Disadvantages:
• Higher infection risk
• Mobility limitations
• Pseudoaneurysm risk
• AV fistula formation
• Retroperitoneal hemorrhage if puncture occurs above the inguinal ligament
The ideal target is the common femoral artery over the femoral head, not the superficial femoral artery.
Superficial Femoral Artery
Generally avoided.
Compared with the common femoral artery, the superficial femoral artery is smaller and may carry greater risks of thrombosis and limb ischemia. Ultrasound should always be used to identify the bifurcation and avoid inadvertent SFA cannulation.
Dorsalis Pedis Artery
Advantages:
• Preserves upper extremity access
• Easy compression
• Useful in burns, trauma, dialysis access patients, and patients with extensive upper extremity instrumentation
Disadvantages:
• Small vessel
• Waveform amplification
• Less reliable in peripheral vascular disease
Rarely used, but worth remembering as a rescue site.
How an Arterial Line Actually Works
The catheter itself is only one part of the system.
The complete setup includes:
• Arterial catheter
• Stiff pressure tubing
• Continuous flush system
• Pressure bag inflated to 300 mmHg
• Pressure transducer
• Monitor interface
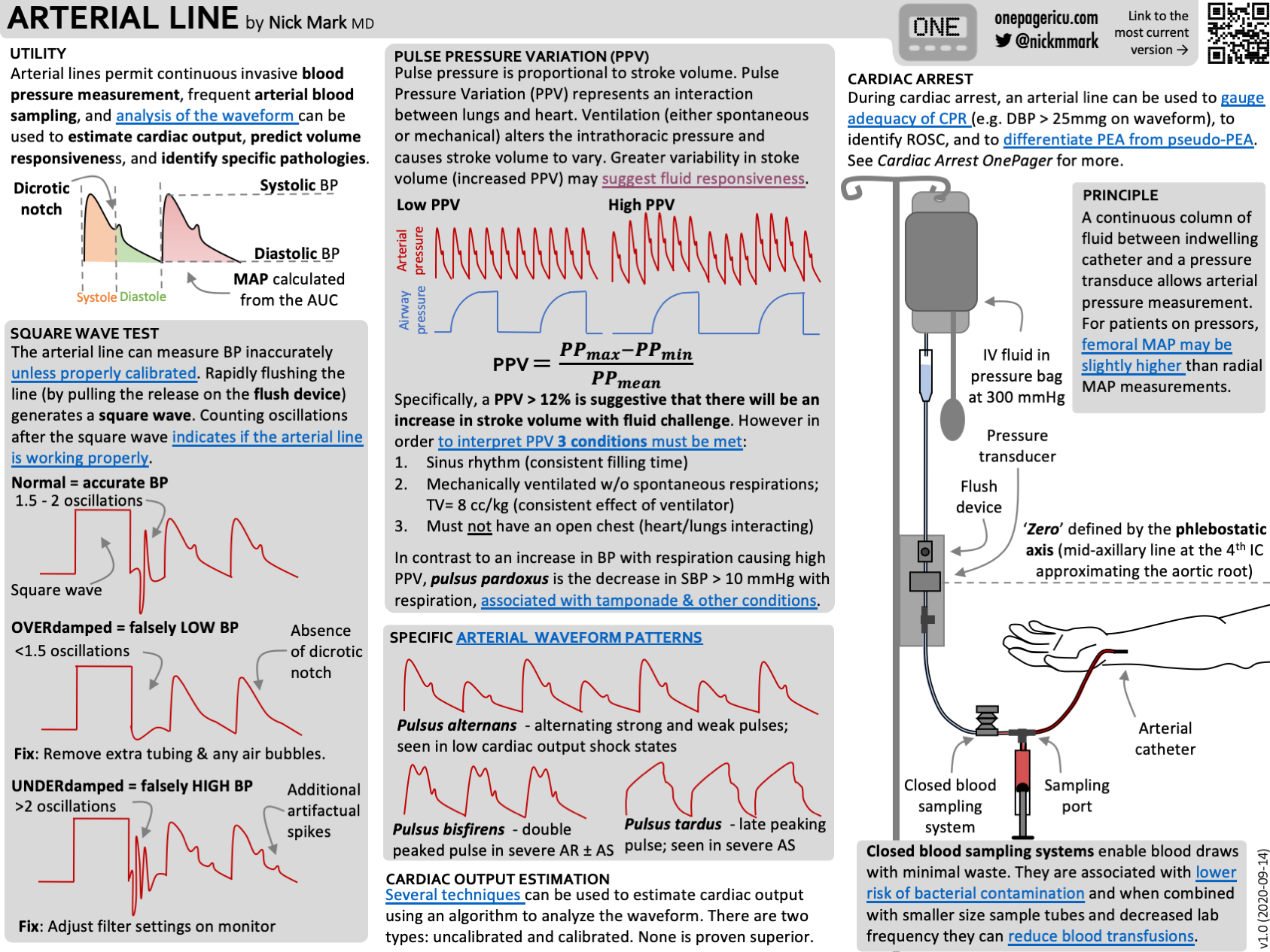
The flush bag maintains a continuous fluid column connecting the arterial circulation to the transducer. Pressure changes within the artery are transmitted through this fluid column to a diaphragm inside the transducer. A Wheatstone bridge converts diaphragm deformation into an electrical signal, producing the arterial waveform displayed on the monitor.
Accurate measurements require:
• Continuous fluid column
• Proper leveling
• Proper zeroing
• Absence of air bubbles
• Adequate flush pressure
Closed Blood Sampling Systems
Modern arterial line systems frequently include closed blood sampling devices.
Benefits include:
• Reduced contamination risk
• Reduced blood waste
• Lower transfusion requirements
Several studies have demonstrated meaningful reductions in iatrogenic blood loss, with some reporting approximately 12% fewer transfusions.
Zeroing and Leveling
Zeroing calibrates the transducer to atmospheric pressure.
Procedure:
Open the transducer to air
Press zero
Re-cap the stopcock
Reconnect to the patient
The transducer should be leveled at the phlebostatic axis, approximately corresponding to the right atrium. Even modest height differences can substantially alter measured pressure.
The Square Wave Test
Every clinician who interprets arterial pressures should understand dynamic response testing.
Procedure:
Activate the fast-flush device
Observe a square-wave plateau
Release the flush
Count oscillations
Normal: 1.5–2 oscillations
Overdamped system:
• Too few oscillations
• Underestimates systolic pressure
• Produces blunted waveform
Common causes:
• Clot
• Kinked catheter
• Air bubbles
• Loose connections
• Low flush pressure
Underdamped system:
• Excessive oscillations
• Overestimates systolic pressure
• Produces spiky waveform
Common causes:
• Excessively compliant tubing
• Catheter whip
• Patient movement
• Resonance effects
• Faulty equipment
Pulse Pressure Variation (PPV)
PPV is one of the most important dynamic measures of fluid responsiveness.
During positive pressure ventilation, changes in intrathoracic pressure alter venous return and ventricular filling. When preload reserve is limited, these changes create measurable swings in pulse pressure.
A PPV greater than approximately 12% suggests fluid responsiveness under ideal conditions.
However, PPV only works reliably when:
• Sinus rhythm is present
• The patient is fully mechanically ventilated
• No spontaneous respiratory effort exists
• Tidal volume is adequate (approximately 8 mL/kg)
• Chest is closed
Most importantly:
Fluid responsiveness means stroke volume would increase if fluid were given.
It does not mean:
• The patient needs fluid
• Giving fluid is beneficial
• Giving fluid is safe
Arterial Lines During Cardiac Arrest
Arterial monitoring provides unique advantages during CPR.
Coronary perfusion pressure is driven primarily during diastole. During CPR, maintaining a diastolic pressure above approximately 25 mmHg is associated with improved chances of ROSC.
Additional advantages:
• Objective pulse assessment
• Immediate recognition of ROSC
• Reduced interruptions in chest compressions
• Improved CPR quality monitoring
Recognizing Important Waveforms
Pulsus Paradoxus
An inspiratory decrease in systolic blood pressure exceeding 10 mmHg.
Associated with:
• Cardiac tamponade
• Constrictive pericarditis
• Severe asthma
• Severe COPD
Pulsus Alternans
Alternating strong and weak arterial pulses.
Usually reflects severe left ventricular systolic dysfunction and low cardiac output states.
Pulsus Bisferiens
Two systolic peaks separated by a midsystolic dip.
Associated with:
• Mixed aortic stenosis and regurgitation
• Hypertrophic obstructive cardiomyopathy
Pulsus Tardus
Delayed systolic upstroke.
Classically seen in severe aortic stenosis.
Common Myths
Do You Need an Allen Test?
Probably not.
The modified Allen test was originally developed for a different purpose and has never demonstrated convincing evidence that it improves safety before radial artery cannulation. Modern ultrasound assessment provides far more useful information.
Did the French Trial Prove Arterial Lines Are Useless?
No.
The trial was designed around an implausibly large mortality reduction. Failure to demonstrate a huge mortality benefit does not mean arterial lines lack clinical value. Monitoring devices generally improve decision making rather than directly reducing mortality. Furthermore, crossover and exclusion rates bias such studies toward null findings.
Do Sick Patients Need Femoral Arterial Lines?
Not necessarily.
While femoral access is often easier during CPR, profound vasoconstriction, or ECMO evaluation, most studies show only modest differences between radial and femoral MAP measurements, often in the range of 3–5 mmHg. Many clinicians routinely manage severe cardiogenic shock and liver transplant patients using radial arterial monitoring with excellent results.
Can Arterial Lines Measure Cardiac Output?
Pulse contour systems estimate cardiac output by analyzing the arterial waveform.
Examples include:
• FloTrac
• LiDCO
• PiCCO
• MostCare
These systems are often useful for trending changes over time but are less reliable for absolute cardiac output measurements. Reported error rates relative to thermodilution commonly range from 20–40%.
Key Takeaways
• Use arterial lines aggressively when patients need them.
• Remove them aggressively once they do not.
• Ultrasound guidance should be routine.
• Lidocaine improves patient comfort, not just during but also after the procedure.
• Understand how to zero, level, and troubleshoot the system yourself.
• Never disable arterial line alarms.
• Radial and ulnar arteries should be first-line sites for most patients.
• Femoral access is an excellent second-line option and often ideal during CPR or ECMO evaluation.
• Brachial, axillary, and dorsalis pedis access remain valuable rescue sites.
• Pulse pressure variation is useful but highly conditional.
• Waveform interpretation provides physiologic information beyond blood pressure alone.
• Monitoring devices help clinicians make better decisions—but the device itself is never a substitute for clinical judgment: its the wizard not the wand.